BY ANISH KOKA
If there was any doubt the academic research enterprise is completely broken, we have an absolute train wreck of a study in one of the many specialty journals of the Journal of the American Medical Association — JAMA Health.
I had no idea the journal even existed until today, but I now know to approach the words printed in this journal to the words printed in supermarket tabloids. You should too!
The paper that was brought to my attention is one that purports to examine the deleterious health effects of Long COVID. A sizable group of intellectuals who are still socially distancing and wearing n95s live in fear of a syndrome that persists long after a person recovers from COVID. There are any number of papers that argue a variety of putative mechanisms for how an acute COVID infection may result in long term health concerns. This particular piece of research that is amplified by the usual credentialed suspects on social media found “increased rates of adverse outcomes over a 1-year period for a PCC (post-COVID conditions) cohort surviving the acute phase of illness.”
In this case PCC (Post-COVID conditions), is the stand-in for Long COVID, and leading commentators use this paper to explicitly state that heart attacks, strokes and other major adverse outcomes doubled in people post-COVID at 1 year…
It is a crazy statement, and anyone regurgitating this has no business commenting on any scientific papers. Let me explain why.
In order to find out about the potential ravages of long COVID researchers need to be able to compare outcomes between those who were infected with COVID and now have long covid to those who were never infected with COVID. At this point finding a large enough group of people that never had covid is impossible, because everyone in the world will have been infected with COVID many, many times. It’s also really hard to define the nebulous long COVID because a study after study finds no clear objective markers of the disease.
The syndrome is defined by a nebulous collection of subjective symptoms COVID survivors feel. In cases like this, an ideal control group is people that think they had COVID, but never tested positive for COVID. This was achieved in this study in the midst of the pandemic which compared self-reported COVID19 infection with sars-cov2 serology results (published in the JAMA network too!) and found that persistent physical long-term symptoms were associated more with the belief of having experienced COVID-19 infection than with having had a positive Sars-COV2 lab test. (The notable exception was loss of smell).
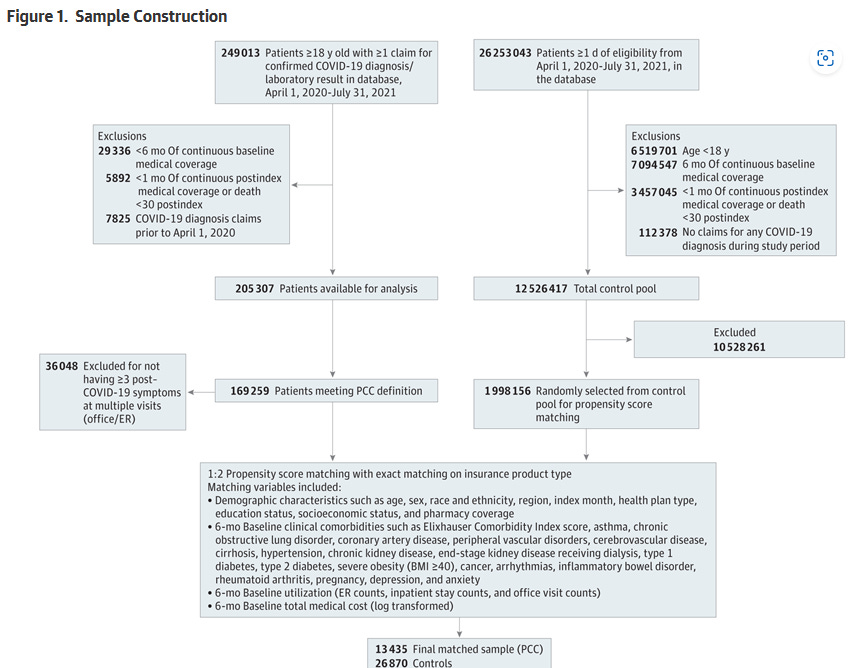
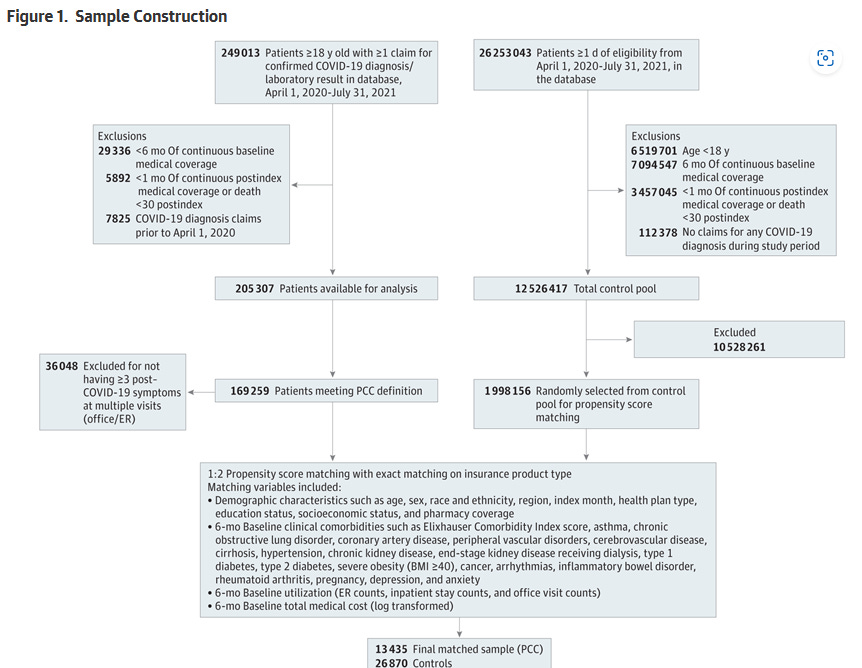
The most recent study in JAMA-Health defines long COVID as patients who had at least 3 diagnoses coded in an electronic medical records claims database in patients who had a prior diagnosis of COVID or a prior COVID positive test. Individuals in the PCC cohort received 3 or more diagnoses for COVID-19 or COVID-19 symptoms across more than 1 visit during weeks 5 to 12 after their defined index date. Essentially everyone with COVID by default makes up the potential PCC sample. Of the 205,307 patients available for analysis with prior COVID, ~36,000 individuals were excluded for not having three or more COVID 19 symptoms at multiple visits 5-12 weeks after the COVID diagnosis. This left ~169,000 patients who continued to have at least three COVID symptoms that met criteria and were defined as having PCC or “longCOVID”.
The authors, and those amplifying this study seem to believe that ~70% of patients with COVID will go on to have chronic symptoms related to COVID. This is an absurd statement that has no basis in reality for anyone who lives in the real world. If it were true, everyone would be confined to their basement as opposed to packing Superbowl stadiums.
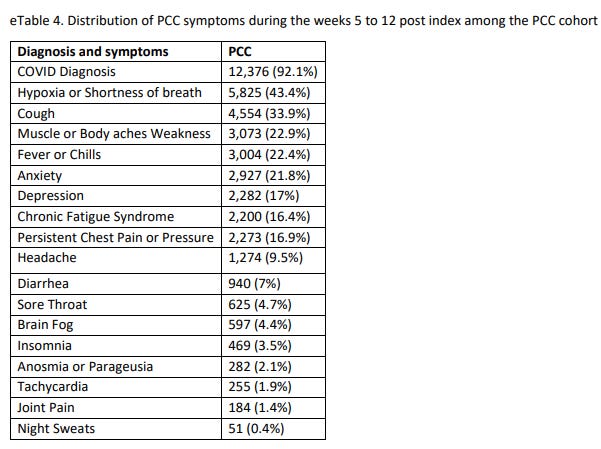
Of the massive list of diagnoses that would qualify a patient to have a chronic covid condition, the authors helpfully provide a distribution of the symptoms that made patients qualify.
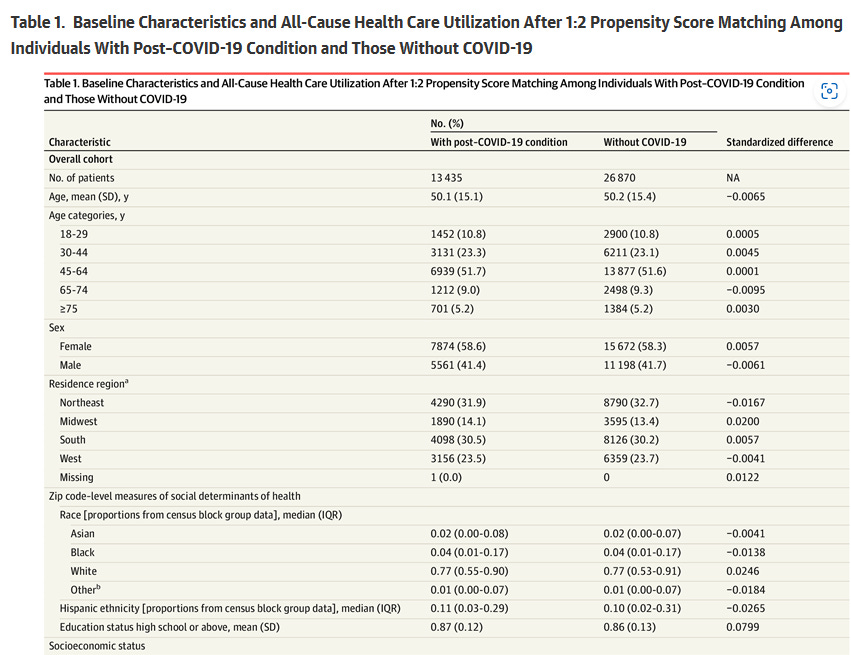
Almost half of the patients still had an ICD10 diagnosis of hypoxemia, and a third had a diagnosis of cough coded 5-12 weeks after having had COVID. Researchers than compare this group of patients to a historical control that consists of patients matched for age, gender, socioeconomic status, and major comorbidities.
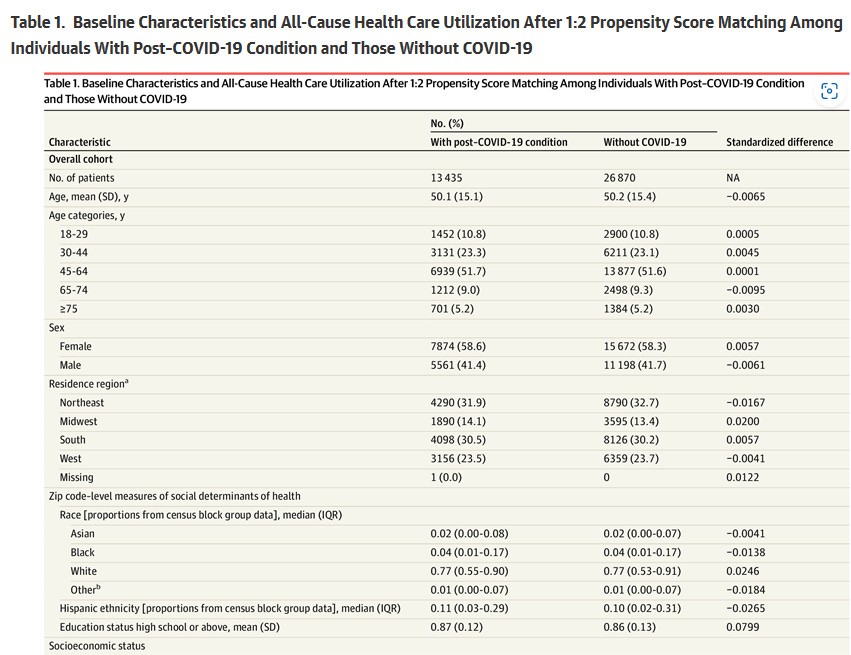
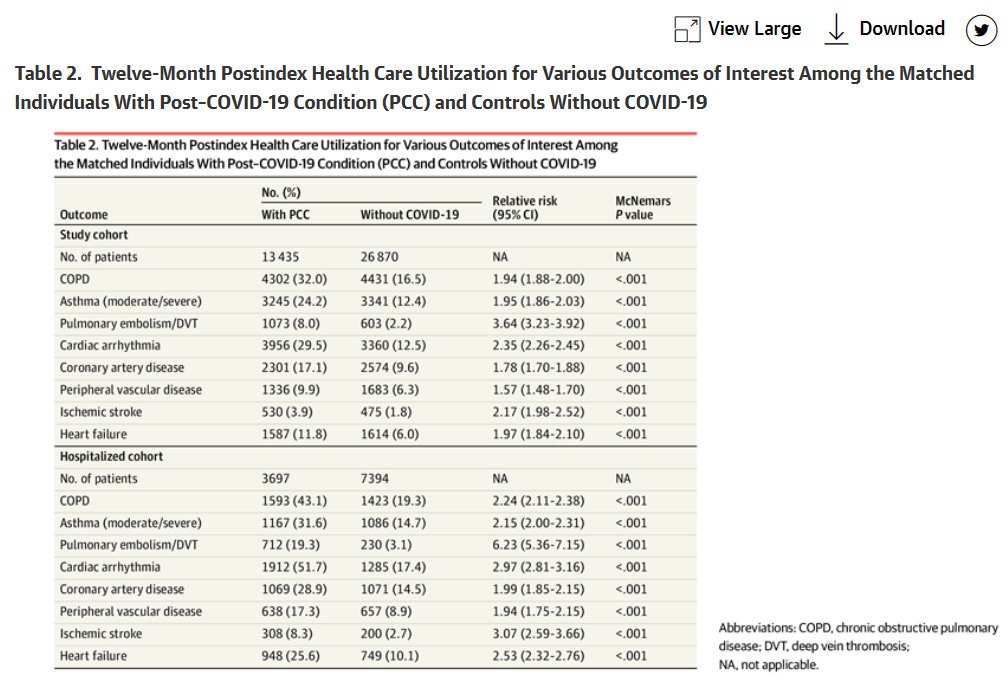
This allowed the researchers to come up with an expected rate of adverse events for a population that did not have COVID, and compare it to observed adverse events in the longCOVID group at 12 months.
The relative risk of every major adverse event is significantly increased in the post COVID group.
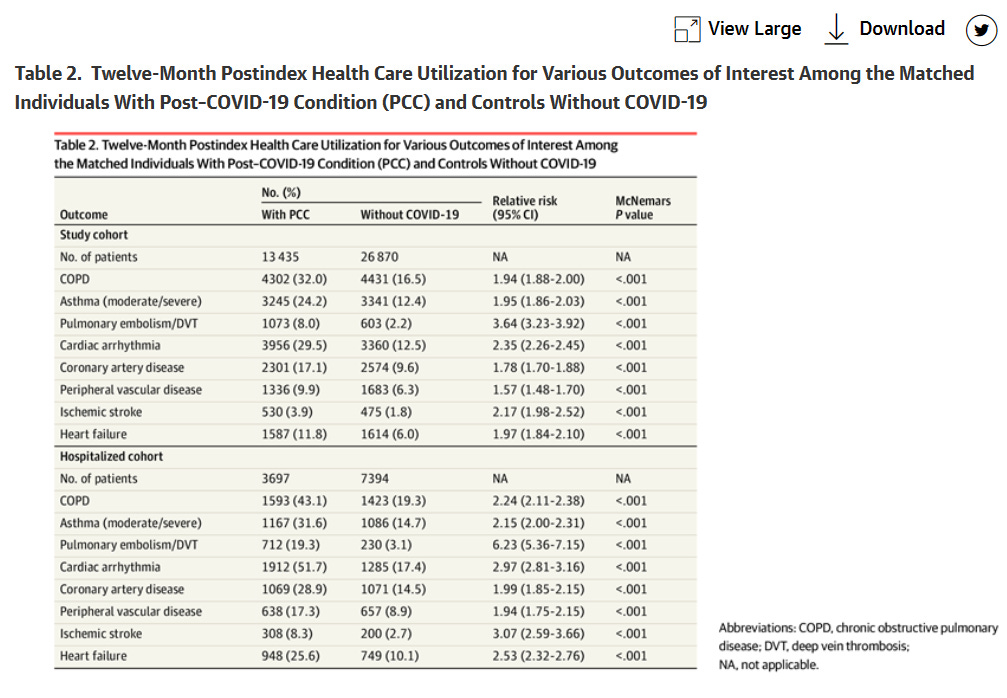
But what does this mean? Does COVID actually increase the risk of getting COPD , coronary disease, and an ischemic stroke by a factor of 2?
NO!
It means that patients who have a diagnosis of shortness of breath or hypoxemia coded in an electronic medical record are more likely to have a diagnosis of COPD placed in the electronic medical record in the 12 months after having had COVID. Vulnerable patients in a population who do not carry any official medical diagnoses are at risk of being hospitalized or falling ill when a novel respiratory virus appears. These same patients are then going to be more likely to have persistent symptoms regardless of whether the virus is a new strain of RSV, influenza, or the novel coronavirus. Patients who are admitted to the hospital with a covid pneumonia are also a lot more likely to be diagnosed with every single outcome that the study authors are looking for!
The COVID research explosion uncovers the dirty secret that much of academic medicine has turned into plumbing large datasets to fabricate clickbait conclusions to serve some ideological purpose. It’s hard to sort this out when the topic relates to a complicated medical topic in a prestigious journal. The default is to believe the conclusions published by credentialed people in big-name journals. But when the public that has had COVID multiple times over is told that 70% of patients who survived covid have long-covid symptoms and are now at twice the risk of every single major cardio/pulmonary/vascular recognized the statement for the lie it clearly is.
One can only hope the public wakes to the generally awful level of research being produced by a vast array of academics on topics well beyond COVID.
Anish Koka is a cardiologist in Philadelphia. Follow him on twitter @anish_koka













{kind=link}
{kind=link}
{kind=link}
{kind=link}